
Why We Chose Oral Placement Therapy to Address AADC Deficiency Speech Problems
The approach combines visual, auditory, and tactile stimulation to improve speech, feeding
Written by |



When I don’t know how to do something, I’m the type of person to go figure it out. YouTube has taught me skills ranging from fixing a leaky faucet to trail running. My wife and I applied the same method when it came to speech therapy training.
Speech seemed like a distant goal for our daughter, Rylae-Ann, who has aromatic l-amino acid decarboxylase (AADC) deficiency. This is because AADC deficiency causes more severe symptoms that take precedence. However, we tried our best to work on speech when we had time. Thankfully, my wife is a special education teacher and has some training, but even she was at a loss in terms of developing a treatment plan for our daughter’s unique case.
When Rylae-Ann was diagnosed at 8 months old, we knew she would have speech problems. We wanted to meet this challenge head-on and begin early intervention. We sought outside assistance at speech therapy clinics, but the doctor told us that Rylae-Ann was still developing, and therefore too young to receive treatment.
It seemed like we were being told to wait until there was a more significant problem before proceeding. This method did not sit well with us, and there was no way we would sit idly by. We found many helpful videos on YouTube, but one led us to a specific form of speech therapy called oral placement therapy, or OPT.
There was no speech intervention guide for AADC deficiency, so we also connected with other rare disease support groups and researched programs that supported cases involving similar symptoms and challenges as our daughter. OPT was mentioned within the groups and seemed like a perfect match.

What is oral placement therapy?
OPT is a speech therapy approach that combines visual, auditory, and tactile stimulation to improve speech and feeding skills. It focuses on all the muscles involved in speech, not just the mouth.
What caught our attention about this program was that it looks at early intervention and offers treatment to young children before they have speech problems. This is exactly what we were looking for.
We visited the website of TalkTools, an organization that provides resources and training for oral motor placement therapy, and appreciated all of the helpful information, much of it free of charge. The site also links to a directory of licensed OPT speech therapists around the world. It encouraged us to take things a step further by enrolling in a program and completing their training courses.
We wanted to learn and apply the strategies directly. The courses aren’t free, and we also needed to pay for equipment sold separately. But doing so empowered us to confidently provide treatment for Rylae-Ann at home. This, combined with our other therapies, led to noticeable improvements by our daughter.
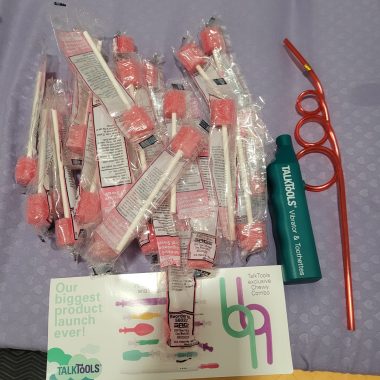
While completing oral placement therapy training, Richard and his wife, Judy, began using the assigned tools with their daughter, Rylae-Ann. (Courtesy of Richard E. Poulin III)
Early intervention and preventive care
TalkTools was founded by Sara Rosenfeld-Johnson, an internationally recognized speech and language pathologist. She also was the teacher for our course.
Rosenfeld-Johnson began our first class by sharing a story about a baby with Down syndrome. The baby was experiencing feeding difficulties but was not receiving speech therapy intervention due to young age. Rosenfeld-Johnson was surprised about this and felt action should be happening from birth, especially when it was known that the child would have speech difficulties later. This story felt almost identical to what my wife and I had experienced.
In a 1997 article in Advance Magazine, titled “The Oral-Motor Myths of Down Syndrome,” Rosenfeld-Johnson explained how the facial features of a child with Down syndrome are not a symptom of the disease but a manifestation of not taking early action, and therefore allowing the body to develop the characteristic “myths” of Down syndrome. The stereotypical characteristics were not apparent in the cases she had worked with, because OPT uses an early intervention and prevention approach.
The goal of OPT is to prevent the symptoms from occurring in the first year of life. So, although children cannot yet speak, speech therapy is used. OPT relies on understanding the mechanics and physiology of the mouth to achieve certain goals. These goals may be initially related to sucking and feeding, but the same muscles are used for speech.
We began when Rylae-Ann was 8 months old, but it should have started when she was born. By beginning sooner, mothers of newborns with AADC deficiency can experience successful breastfeeding, which leads to improved feeding for toddlers. They wouldn’t have to worry about weight gain or providing their child with a feeding tube. Eventually, speech has a greater likelihood of happening.

Rylae-Ann improved her feeding due to oral placement therapy, which eventually led to speech. (Courtesy of Richard E. Poulin III)
OPT for special needs
Another reason we believed OPT was the best match for our daughter is because it aids several special needs cases, including Down syndrome, cerebral palsy, autism spectrum disorder, attention-deficit/hyperactivity disorder, and those with motor-sensory impairments. This list featured similar challenges faced by our daughter. In addition, the multisensory approach aligned with our experience with early education and learning support curriculums.
Special needs children benefit from tactile and proprioceptive components, which are very different from traditional speech therapy. In special education, educators use a similar technique of combining multiple senses and learning styles to reach individual children. So while we were working on speech, we also improved her senses, overall articular awareness, placement, stability, and muscle memory.
Our results
The results for us began slowly, but we did not rush the sequence. Rylae-Ann’s first milestone was allowing us to use the tools in and around her mouth to help her build muscle awareness. Her sensory processing issues did not make this an easy task, but she did it.
Then, she quickly learned to drink from a straw and blow bubbles. This was a huge leap, and the progress continued.
After she had gene therapy, the progress was even quicker, which I believe was due to early intervention with OPT speech therapy.
Success with this method strengthened our resolve to support our daughter and other parents who want to do the same with their children. Oral placement therapy is one component of speech and language. To maximize results, it should be led by a licensed therapist and not done in isolation. All paramedical therapies work together to allow a child to make the most significant progress possible. As always, consult your healthcare team before making any treatment or therapy decisions.

Thanks to Rylae-Ann’s dedication and hard work during speech therapy, she is able to eat independently while talking with her friends at lunch. (Courtesy of Richard E. Poulin III)
Note: AADC News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. The opinions expressed in this column are not those of AADC News or its parent company, Bionews, and are intended to spark discussion about issues pertaining to aromatic l-amino acid decarboxylase deficiency.
Leave a comment
Fill in the required fields to post. Your email address will not be published.